Rough Home Test for Peripheral Artery Disease Using BP Monitor
Procedure:
- With patient on a bed, take the BP with the left ankle, being careful to elevate the ankle to same level as the heart. Record the reading.
- Same for right ankle.
- Now left wrist. Leave the patient lying down (avoid making him move).
- Finally, right wrist.
- Take the higher systolic reading for the ankles.
- Take the higher systolic reading for the wrists.
- Divide the ankle number by the wrist number. This is called the Ankle Brachial Index (ABI)
Evaluation:
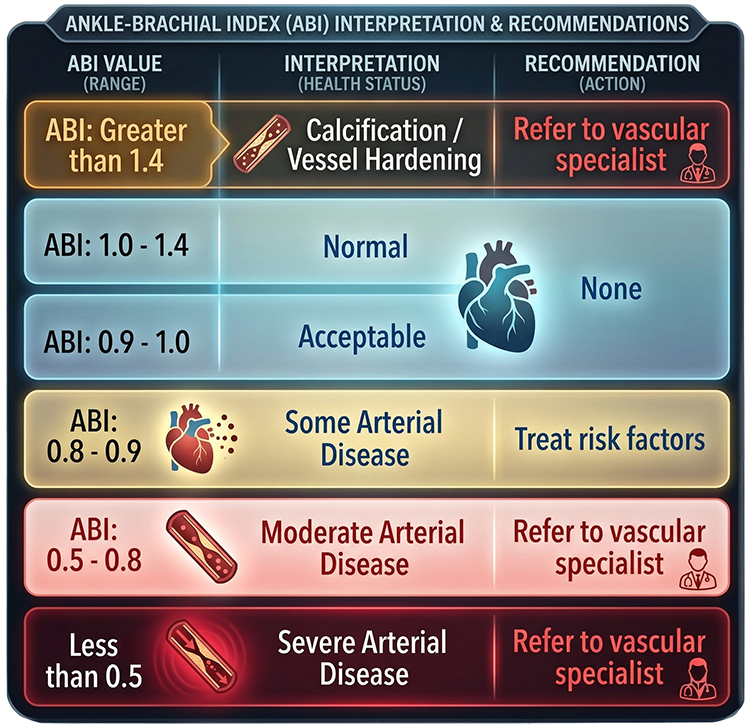
The ankle readings are expected to be higher, because the arteries in the legs are narrower. An ABI of 1.0 to 1.4 is considered normal. If the ABI is lower than 1.0, it indicates Peripheral Arterial Disease (atherosclerosis or plaque buildup, especially affecting legs). Due to plaque constricting the arteries, the blood pressure that reaches the legs is too low. The cells and nerves in the legs, feet, and toes don’t receive enough blood, therefore not enough oxygen. This can cause cell or nerve death, or inability to heal common wounds.
If the ABI is above 1.4, it indicates Hardening of the Arteries (arteriosclerosis, in which the arterial walls have become inflexible due to age, chronic high blood pressure, or severely calcified plaque). Much less blood is reaching the legs, but the BP Monitor is tricked into a false higher systolic reading. BP monitors work by applying pressure until the point that blood flow is stopped by the cuff (or in reverse, when blood flow resumes). If the arteries are hard, that hardness resists the pressure applied by the cuff, making the BP in the ankle read higher than the wrist. And why is there no similar distortion in the wrist reading? Wrist BP is based on the radial artery, which is the artery least susceptible to hardening.
If ABI is above 1.4 or below 0.9, the patient should be advised to undergo more extensive tests with a vascular specialist, and to immediately make lifestyle changes, failing which further decline is inevitable.
If there is a persistent 10% or more difference between left and right readings for either ankle or wrist, the suspicion is lateralized peripheral arterial disease. More extensive tests should also be recommended.
Nattokinase is an enzyme produced by fermenting natto beans. A sufficient amount of Nattokinase can help dissolve plaque and possibly calcified deposits, thus reversing atherosclerosis. In a Chinese retrospective study, a daily dose of 10,800 Fibrinolytic Units, about 540 mg, was administrered to over 1000 subjects with mild symptoms of atherosclerosis (https://pmc.ncbi.nlm.nih.gov/articles/PMC9441630/). After 12 months, about 65% of the study subjects showed significant improvement (lessening) of common carotid artery intima-media (the lipid “phlegm” that turns into calcified deposits) and carotid plaque volume itself. Nattokinase also demonstrated a strong lipid-reducing effect.
When combined with Vitamin K2 and aspirin supplementation, all the improvements were even greater, up to a 60% reduction. It is important to emphasize that other studies using lower doses did not demonstrate any benefit, and that commercial preparations of Nattokinase supplement are somewhat unreliable as to FU claims. However, there has not been any adverse reaction to Nattokinase doses in the vicinity of 10,800, so individuals with atherosclerosis might wish to consider Nattokinase as a “nothing to lose” strategy.
Unfortunately, there are no known plans to conduct a double-blind, placebo-controlled trial of Nattokinase as plaque-reducer or for lipid reduction. A highly-successful trial would not benefit any likely research donor financially, and would financially and reputationally harm pharmaceuticals, some hospitals, many doctors, and the Medical Establishment.